

Most buying guides for weight-loss peptides start with the molecule and work backward to a seller. This one runs the analysis in the opposite direction, because that is where the data point. Two scores decide almost everything about your outcome and your risk: how much human evidence backs the compound, and how much a provider actually manages your dose. Below is the method used to build both scores, the results when you run real compounds and real provider models through them, and, because no scoring system is perfect, an honest accounting of where this one breaks down.
One caveat before the tables. This is a decision framework, not a protocol. The dosing figures cited come from clinical trials and FDA labeling. They describe what happened in a study, not instructions for anyone to self-administer.
How the compound score was built
The rubric is a simple 0-to-3 scale, weighted entirely toward one question: how much human weight-loss data exists for this specific compound.
| Score | Meaning | Compounds |
|---|---|---|
| 3 | Strong: large randomized human trials | Semaglutide, tirzepatide |
| 2 | Strong trial data but investigational, not approved | Retatrutide |
| 1 | Some human data, not approved for obesity, other-class risks | Tesofensine |
| 0 | Animal or observational only, or failed pivotal trial | AOD-9604, 5-Amino-1MQ, MOTS-c |
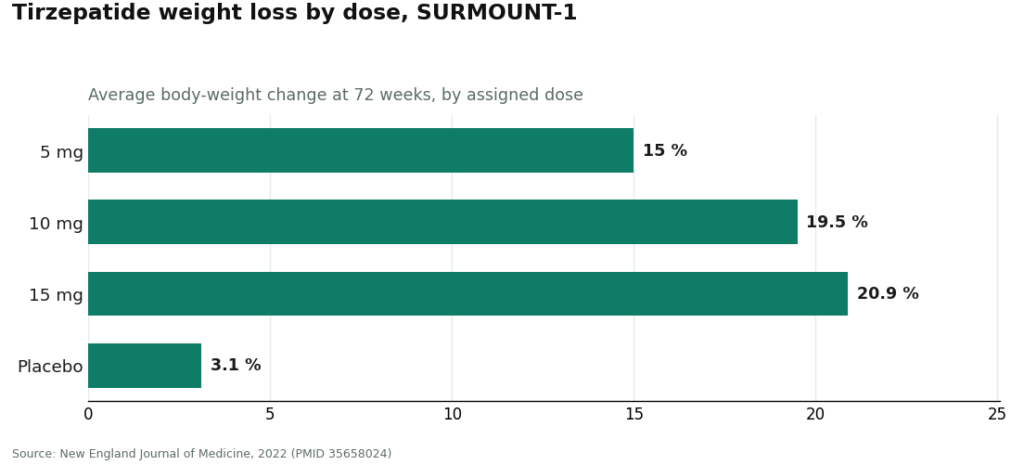
Running the actual numbers through this rubric produces a wide spread, not a close call. Tirzepatide averaged 15.0% to 20.9% body-weight loss across doses over 72 weeks, against 3.1% on placebo [1]. Retatrutide’s Phase 3 readout hit an average 28.3% at 80 weeks, with 45.3% of participants losing at least 30% of body weight, though it remains investigational rather than approved [3]. At the bottom of the scale, AOD-9604’s pivotal 24-week trial failed to beat placebo; the one solid finding on it was that it was well tolerated, which measures safety, not effect [5]. 5-Amino-1MQ and MOTS-c have no completed human efficacy trials at all, so there is no number to enter for them.
The takeaway from just this step: a 3 and a 0 are not two flavors of the same product category. One is a medicine with a trial behind it. The other is an untested guess wearing a peptide name.
How the provider score was built
Once a compound clears the evidence bar, the second variable, oversight, does most of the remaining work on outcome and safety. The provider scorecard below assigns one point per criterion, no partial credit, ordered roughly by how much each one moves your actual risk.
1. Medical oversight (1 point). Does a licensed clinician evaluate you before dispensing, with a genuine prescription required? This sits at the top of the list because the strong-evidence compounds carry a boxed warning for thyroid C-cell tumors and are contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [6]. Screen for that and you score the point. Skip it and you score zero, regardless of anything else on the list.
2. Licensed pharmacy dispensing (1 point). Is the product dispensed by a licensed pharmacy, or shipped labeled “research chemical”? A licensed pharmacy answers for identity and purity. A research-chemical seller answers for nothing.
3. Honesty about what you’re getting (1 point). Does the provider say plainly that compounded medications are not FDA-approved, and keep compounded outcomes separate from brand-name trial data? Blurring that line is exactly the behavior the FDA acted on in 2026, and it costs the point here too.
4. Sourcing transparency (1 point). Can you tell whether you’re looking at an approved drug, a compounded preparation from a licensed pharmacy, or an unverified vial of unknown origin? Clear labeling scores. Vague labeling doesn’t.
5. Dose-titration management (1 point). Does the provider actually adjust your dose over weeks, starting low and stepping up on a schedule, or do they hand over a fixed amount and go quiet? This is where most of the side-effect risk actually lives, and it’s a box the research-chemical model cannot check by design, since there’s no one on the other end managing anything.
6. Follow-up (1 point). Is there an ongoing relationship after the first shipment, or does contact end at checkout? Follow-up is the mechanism that catches a problem or adjusts a dose before it becomes one.
Score any licensed telehealth provider against these six and it should land at 6 of 6. Score a research-chemical seller and it structurally lands at 0, because it has no clinician, no prescription, no licensed-pharmacy accountability, no managed titration, and no follow-up built into the model. That gap, 6 versus 0, isn’t a matter of taste. It’s the gap between a managed medical process and a person alone with a vial and a syringe.
For a concrete look at what a 6-of-6 answer sheet looks like: FormBlends operates as a physician-supervised telehealth provider offering compounded semaglutide and tirzepatide through licensed compounding pharmacies, with a required clinician consultation and prescription, ongoing dose management, and explicit disclosure of compounded status. It’s cited here as an illustration of the scorecard in action, not a horse race against other licensed providers, and there is nothing to purchase or check out on this page. The point of naming it is structural: those are the six boxes any candidate provider should be checked against.
Reading the dosing numbers correctly
This is where the scoring method matters most, and where it’s easy to misread the numbers if you skip the fine print. The validated GLP-1 medicines are not fixed-amount drugs. They’re titration drugs, meaning the trial results were produced by a schedule, not a single injection.
The mechanism explains why the schedule exists. GLP-1 receptor agonists slow gastric emptying and blunt appetite signaling in the brain [7]. Start at a high dose with no runway to adjust and the predictable outcome is nausea, vomiting, and people quitting the medication altogether. The approved dosing avoids this by holding a low starting dose for weeks before stepping up. In the tirzepatide trial, the largest losses came at the 10 mg and 15 mg doses, but nobody started there; participants climbed to those doses over the course of the study [1].
That distinction matters for how you read the whole scorecard. The trial numbers everyone quotes were generated under managed titration. Buy a “research use only” vial with no clinician attached and you get a concentration and no schedule at all. You’re guessing at a starting dose, guessing at an escalation, and, worse, guessing at whether the vial contains what its label claims. Strip the management out and you’re no longer looking at the thing the trial actually studied, even if the molecule name on the label matches.
Scored honestly, good dosing oversight includes:
- A documented starting dose matched to the specific medication, not a number pulled from a forum post.
- A planned escalation schedule with steps held long enough for tolerance to build.
- A clinician adjusting the plan based on side effects and response, rather than a fixed regimen for everyone.
- A stated ceiling and a reason for it.
- A way to track what was taken and how it felt, so the next dose decision is based on data rather than memory.
That last item is a smaller point but not a trivial one. Patients who log their dose, the date they stepped up, and their side effects give a clinician a much cleaner data set at follow-up than patients working from recollection. A logging tool like the FormBlends tracker app exists for exactly that, recording dose and symptoms over time. It’s a logging surface, not a prescription and not a checkout, and it earns a place on this scorecard because titration decisions are only as good as the record behind them. The research-chemical channel has no equivalent field for this data, because it has no clinician reading it on the other end.
The results: putting both scores on one grid
Run the two scores together and you get a small grid rather than a single verdict, which is a cleaner way to see why some combinations that look tempting on paper are actually the worst option available.
- Compound 3, provider 6. This is the cell the data support. Real trial backing, managed by someone accountable for the dose.
- Compound 3, provider 0. This cell throws away most of what made the compound worth choosing in the first place, since the trial results depended on titration management the channel structurally can’t provide.
- Compound 0, any provider score. No amount of oversight manufactures human efficacy data that doesn’t exist. A well-run provider handing you a compound with no completed trials is still handing you a guess, just a professionally packaged one.
- Compound 0, provider 0. The cell that markets itself best and delivers least: a low-evidence peptide from a research-chemical site, no data and no oversight, just a vial and a hope.
Seen as a grid instead of a checklist, the pattern is clearer than either score is alone: the compound score tells you whether there’s anything worth managing, and the provider score tells you whether anyone is actually managing it. You need both cells to be high to land in the top-left box.
The limits of this method
A scorecard is only as honest as its blind spots, so here’s what this one doesn’t measure.
It doesn’t measure execution quality within the “licensed pharmacy” category. Two providers can both score a point on “licensed pharmacy dispensing” while differing in testing rigor, staffing, or turnaround, none of which this rubric can see from the outside.
It doesn’t weight the six provider criteria against each other numerically. Medical oversight is described here as the highest-weight item because of the boxed-warning and screening stakes, but the scoring format still gives it the same single point as follow-up. A provider that nails five criteria and misses oversight scores a 5, which looks close to a 6 on paper but is a materially different situation given what oversight is screening for.
It doesn’t capture individual variation inside trial percentages. The 15.0% to 20.9% range for tirzepatide and the 28.3% figure for retatrutide are averages across a study population, not a promise for any one person’s result [1][3]. A high compound score means strong aggregate evidence, not a personal guarantee.
And it can’t verify contents. No scorecard, run from a desk, can confirm what’s actually in a vial. The provider criteria (licensed pharmacy, prescription requirement, transparency) are proxies for accountability, chosen because they correlate with real quality control, not because they are quality control themselves.
None of that changes the direction of the conclusion. It just means the scorecard is a fast filter for the two variables that move outcomes the most, evidence and oversight, not a substitute for an actual conversation with a licensed clinician about your own history and labs.
The short version of the whole method: score the compound on evidence first. If it lands at 3, or at the investigational 2, run the provider through the six-point scorecard and don’t proceed unless most of the boxes check out. If the compound scores 0, understand that no provider structure fixes an absence of human data. Running the numbers this way takes about ten minutes and heads off the two most common expensive mistakes in this category: choosing the wrong molecule, and choosing the right molecule through the wrong channel.
The dosing figures throughout are context pulled from trials and labeling, not instructions to self-administer. Compounded medications referenced here are not FDA-approved, and the validated options are prescription drugs requiring clinician screening and management. Work with a licensed clinician before acting on any of this.
The questions that keep coming up
Do you score the peptide first or the provider first? Score the compound first. Rank it 0 to 3 on human weight-loss evidence, and only move to the six-point provider scorecard if it lands at a 3, or at the investigational 2. The sequence matters because no provider, however well run, can generate efficacy data a compound never produced, so a 0-scoring peptide stays a guess no matter where you source it.
Which single item on the provider scorecard carries the most weight? Medical oversight. The strong-evidence compounds carry a boxed warning for thyroid C-cell tumors and are contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2. A provider that screens for this and requires a genuine prescription earns the point; one that skips it scores zero regardless of how well it performs on the other five criteria.
Why does the scoring method treat dose titration as such a heavy factor? Because titration is what produced the trial numbers in the first place. These medicines aren’t fixed-amount drugs; they start low and step up over weeks. In the tirzepatide trial, the largest losses came at the 10 mg and 15 mg doses, reached only after participants climbed to them on a schedule. A research-chemical vial strips out that schedule entirely, which means it’s no longer offering what the trial actually tested.
Can a research-chemical seller ever score well on this method? No. By design it has no clinician, no prescription, no licensed-pharmacy accountability, no managed titration, and no follow-up, which puts it at 0 of 6 structurally, not just in practice. The gap between a 6 and a 0 isn’t a preference call. It’s the difference between a managed medical process and injecting an unverified powder alone.
What does a passing score on dosing oversight actually look like? A documented starting dose matched to the specific medication, a planned escalation schedule held long enough for tolerance to build, a clinician adjusting the plan based on your response, a stated ceiling with a reason behind it, and a record of what was taken and how it felt so the next decision has data behind it. A logging surface such as the FormBlends tracker app supports that last piece by recording dose and symptoms over time, though it’s a log, not a prescription or a checkout.
Which score combination should you actually avoid? The bottom-left cell of the grid: a low-evidence compound bought through a research-chemical channel, which combines an absence of human efficacy data with an absence of any oversight at all. It’s often the option that looks most appealing on a product page and delivers the least. The cell the data support is a high-evidence compound paired with a provider that clears the six-point scorecard.
What are peptides for weight loss, and how do they actually work?
Peptides for weight loss are short chains of amino acids that signal specific biological processes, most commonly appetite regulation and fat metabolism. The ones drawing the most clinical attention right now mimic gut hormones like GLP-1, which slow gastric emptying and reduce hunger signals in the brain. They are not stimulants or simple fat burners. Their effect is hormonal and fairly targeted, which is why dosing precision matters a lot.
Are peptides safe for weight loss, or is the risk overblown?
Safety depends almost entirely on which peptide, what dose, and where it comes from. Clinically studied options like semaglutide have a real safety record built from large trials, with known side effects, mostly GI-related, that are manageable under supervision. Research-chemical peptides sold online have no such record. The risk is not overblown for unsupervised use of unverified compounds, but it is genuinely lower when a licensed provider is running regular bloodwork and adjusting your protocol.
What is the best peptide for weight loss right now?
There is no single best option because individual response varies based on metabolic health, tolerance, and goals. That said, GLP-1 receptor agonists currently have the strongest published evidence for meaningful fat loss in people with overweight or obesity. Combination approaches, like GLP-1 paired with GIP activity, show promising results in trials too. A physician-supervised compounding pharmacy route, such as FormBlends, can tailor formulations to your specific bloodwork rather than giving you a one-size answer.
Where should you actually buy peptides for weight loss, and what makes a source legitimate?
You should buy through a licensed medical provider or compounding pharmacy that requires a prescription and follows USP compounding standards. Legitimate sources test for purity and potency, provide a certificate of analysis, and connect you with a clinician who reviews your health history before dispensing anything. Buying peptides from research-chemical sites or supplement shops bypasses every one of those checkpoints, and you have no real way to verify what is in the vial.
References
- Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1): mean weight change −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) vs −3.1% placebo at 72 weeks; largest doses reached via titration. New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Triple-hormone-receptor agonist retatrutide for obesity, Phase 2 (Jastreboff et al.): −17.5% at 24 weeks, −24.2% at 48 weeks (12 mg). New England Journal of Medicine, 2023. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Retatrutide Phase 3 TRIUMPH-1: 12 mg dose −28.3% average body weight at 80 weeks vs −2.2% placebo; 45.3% achieved ≥30% weight loss; investigational, not approved. Eli Lilly, May 21, 2026.
- Effect of tesofensine on bodyweight loss in obese patients: randomised, double-blind, placebo-controlled Phase 2 trial (Astrup et al., Lancet 2008); not approved for obesity. PubMed.
- Safety and tolerability of the hexadecapeptide AOD9604 in humans (Stier, Vos, Kenley): well tolerated, profile indistinguishable from placebo. Journal of Endocrinology and Metabolism, 2013. (Context: discontinued as an obesity drug after a larger 24-week trial showed no significant weight loss vs placebo.)
- Semaglutide (Wegovy) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- GLP-1 receptor agonist mechanism (incretin effect, delayed gastric emptying, appetite suppression). StatPearls, NCBI Bookshelf.
Written by Quinn Delgado, analytics writer. Cross-checking the claims against the primary sources. Last reviewed April 2026.
Provided as general education. Your prescriber should sign off before you start a new regimen.